
Abstract
Background
Diffuse type adenocarcinoma and, more specifically, signet ring cell carcinoma (SRCC) of the stomach and gastroesophageal junction (GEJ) have a poor prognosis and the value of neoadjuvant chemo(radio)therapy (nCRT) is unclear.
Methods
All patients who underwent surgery for diffuse type gastric and GEJ carcinoma between 2004 and 2015 were retrospectively included from the Netherlands Cancer Registry. The primary outcome was overall survival after surgery. Kaplan–Meier curves were plotted. Furthermore, multivariable Poisson and Cox regressions were performed, correcting for confounders. To comply with the Cox regression proportional hazard assumption, gastric cancer survival was split into two groups, i.e. <90 days and >90 days, postoperatively by adding an interaction variable.
Results
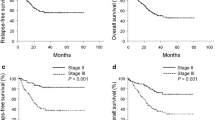
Analyses included 2046 patients with diffuse type cancer: 1728 gastric cancers (50% SRCC) and 318 GEJ cancers (39% SRCC). In the gastric cancer group, 49% received neoadjuvant chemotherapy (nCT) and 51% received primary surgery (PS). All-cause mortality within 90 days postoperatively was lower after nCT (hazard ratio [HR] 0.29, 95% confidence interval [CI] 0.20–0.44; p < 0.001). Also after 90 days, mortality was lower in the nCT group (HR for the interaction variable 2.84, 95% CI 1.87–4.30, p < 0.001; total HR 0.29*2.84 = 0.84). In the GEJ group, 38% received nCT, 22% received nCRT, and 39% received PS. All-cause mortality was lower after nCT (HR 0.63, 95% CI 0.43–0.93; p = 0.020) compared with PS. The nCRT group was removed from the Cox regression analysis since the Kaplan–Meier curves of nCRT and PS intersected. The results for gastric and GEJ carcinomas were similar between the SRCC and non-SRCC subgroups.
Conclusion
For gastric and GEJ diffuse type cancer, including SRCC, nCT was associated with increased survival.



Similar content being viewed by others


References
Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. An attempt at a histoclinical classification. Acta Pathol Microbiol Scand. 1965;64:31–49. https://doi.org/10.1111/apm.1965.64.1.31.
Jass JR, Sobin LH, Watanabe H. The World Health Organization’s histologic classification of gastrointestinal tumors. A commentary on the second edition. Cancer. 1990;66:2162–7. https://doi.org/10.1002/1097-0142(19901115)66:10%3c2162::aid-cncr2820661020%3e3.0.co;2-n.
Dassen AE, Dikken JL, Bosscha K, Wouters MWJM, Cats A, Van De Velde CJH, et al. Gastric cancer: decreasing incidence but stable survival in the Netherlands. Acta Oncol (Madr). 2014;53:138–42. https://doi.org/10.3109/0284186X.2013.789139.
Dikken JL, Lemmens VE, Wouters MWJM, Wijnhoven BP, Siersema PD, Nieuwenhuijzen GA, et al. Increased incidence and survival for oesophageal cancer but not for gastric cardia cancer in the Netherlands. Eur J Cancer. 2012;48:1624–32. https://doi.org/10.1016/j.ejca.2012.01.009.
Cunningham D, Allum WWH, Stenning SSP, Thompson JNJ, Van de Velde CJH, Nicolson M, Scarffe J, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11–20. https://doi.org/10.1056/NEJMoa055531.
Piessen G, Messager M, Leteurtre E, Jean-Pierre T, Mariette C. Signet ring cell histology is an independent predictor of poor prognosis in gastric adenocarcinoma regardless of tumoral clinical presentation. Ann Surg. 2009;250:878–87. https://doi.org/10.1097/SLA.0b013e3181b21c7b.
Kim JP, Kim SC, Yang HK. Prognostic significance of signet ring cell carcinoma of the stomach. Surg Oncol. 1994;3:221–7.
Li C, Kim S, Lai JF, Hyung WJ, Choi WH, Choi SH, et al. Advanced gastric carcinoma with signet ring cell histology. Oncology. 2007;72:64–8. https://doi.org/10.1159/000111096.
Yokota T, Kunii Y, Teshima S, Yamada Y, Saito T, Kikuchi S, et al. Signet ring cell carcinoma of the stomach: a clinicopathological comparison with the other histological types. Tohoku J Exp Med. 1998;186:121–30. https://doi.org/10.1620/tjem.186.121.
Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393:1948–57. https://doi.org/10.1016/S0140-6736(18)32557-1.
Nafteux PR, Lerut TE, Villeneuve PJ, Dhaenens JM, De Hertogh G, Moons J, et al. Signet ring cells in esophageal and gastroesophageal junction carcinomas have a more aggressive biological behavior. Ann Surg. 2014;260:1023–9. https://doi.org/10.1097/SLA.0000000000000689.
van der Kaaij RT, Koemans WJ, van Putten M, Snaebjornsson P, Luijten JC, van Dieren JM, et al. A population-based study on intestinal and diffuse type adenocarcinoma of the oesophagus and stomach in The Netherlands between 1989 and 2015. Eur J Cancer. 2020;130:23–31. https://doi.org/10.1016/j.ejca.2020.02.017.
Messager M, Lefevre JH, Pichot-Delahaye V, Souadka A, Piessen G, Mariette C. The impact of perioperative chemotherapy on survival in patients with gastric signet ring cell adenocarcinoma: a multicenter comparative study. Ann Surg. 2011;254:684–93. https://doi.org/10.1097/SLA.0b013e3182352647.
Ugo D, Agnes A, Grieco M, Biondi A, Persiani R. Global updates in the treatment of gastric cancer: a systematic review. Part 2: perioperative management, multimodal therapies, new technologies, standardization of the surgical treatment and educational aspects. Updates Surg. 2020;72:12–8.
Moehler M, Baltin CTH, Ebert M, Fischbach W, Gockel I, Grenacher L, et al. International comparison of the German evidence-based S3-guidelines on the diagnosis and multimodal treatment of early and locally advanced gastric cancer, including adenocarcinoma of the lower esophagus. Gastric Cancer. 2015;18:550–63. https://doi.org/10.1007/s10120-014-0403-x.
Hamilton SR, Aaltonen LA. World health organization classification of tumours pathology and genetics of tumours of the digestive system. Lyon: International Agency Res for Research on Cancer (IARC Press); 2000.
Stichting PALGA. Landelijke PALGA Protocol: Oesofagus-Maagcarcinoom 2019:versie 45.
Mariette C, Carneiro F, Grabsch HI, van der Post RS, Allum W, de Manzoni G, et al. Consensus on the pathological definition and classification of poorly cohesive gastric carcinoma. Gastric Cancer. 2019;22(1):1–9. https://doi.org/10.1007/s10120-018-0868-0.
Verhage RJJ, Zandvoort HJA, Ten Kate FJW, Van Hillegersberg R. How to define a positive circumferential resection margin in T3 adenocarcinoma of the esophagus. Am J Surg Pathol. 2011;35:919–26. https://doi.org/10.1097/PAS.0b013e31821a5692.
Washington K. 7th edition of the AJCC cancer staging manual: Stomach. Ann Surg Oncol. 2010;17:3077–9. https://doi.org/10.1245/s10434-010-1362-z.
Integraal Kankercentrum Nederland. Richtlijn Diagnostiek, behandeling en follow-up van het maagcarcinoom 2009.
Integraal Kankercentrum Nederland. Diagnostiek, behandeling en follow-up van het maagcarcinoom 2016:1–7. http://www.oncoline.nl/uploaded/docs/Maagcarcinoom/Richtlijnmaagcarcinoom.pdf.
van Hagen P, Hulshof MCCM, van Lanschot JJB, Steyerberg EWW, van Berge Henegouwen MI, Wijnhoven BPLP, et al. Preoperative chemoradiotherapy for Esophageal or junctional cancer. N Engl J Med. 2012;366:2074–84. https://doi.org/10.1056/NEJMoa1112088.
Van Der Kruijssen DEW, Brouwer NPM, Van Der Kuil AJS, Verhoeven RHA, Elias SG, Vink GR, et al. Interaction between primary tumor resection, primary tumor location, and survival in synchronous metastatic colorectal cancer: a population-based study. Am J Clin Oncol Cancer Clin Trials. 2021;44:315–24. https://doi.org/10.1097/COC.0000000000000823.
Modest DP, Ricard I, Stintzing S, Fischer von Weikersthal L, Decker T, Kiani A, et al. Evaluation of survival across several treatment lines in metastatic colorectal cancer: analysis of the FIRE-3 trial (AIO KRK0306). Eur J Cancer. 2017;84:262–9.
Walters DM, McMurry TL, Isbell JM, Stukenborg GJ, Kozower BD. Understanding mortality as a quality indicator after esophagectomy. Ann Thorac Surg. 2014;98:506–12. https://doi.org/10.1016/j.athoracsur.2014.03.041.
Low DE, Alderson D, Cecconello I, Chang AC, Darling GE, D’Journo XB, et al. International consensus on standardization of data collection for complications associated with esophagectomy: esophagectomy complications consensus group (ECCG). Ann Surg. 2015;262:286–94. https://doi.org/10.1097/SLA.0000000000001098.
Baiocchi GL, Giacopuzzi S, Marrelli D, Reim D, Piessen G, Matos da Costa P, et al. International consensus on a complications list after gastrectomy for cancer. Gastric Cancer. 2019;22:172–89. https://doi.org/10.1007/s10120-018-0839-5.
Knol MJ, Le Cessie S, Algra A, Vandenbroucke JP, Groenwold RHH. Overestimation of risk ratios by odds ratios in trials and cohort studies: Alternatives to logistic regression. CMAJ. 2012;184:895–9. https://doi.org/10.1503/cmaj.101715.
Anderson JR, Cain KC, Gelber RD. Analysis of survival by tumor response. J Clin Oncol. 1983;1:710–9. https://doi.org/10.1200/JCO.1983.1.11.710.
Concato J, Peduzzi P, Holford TR, Feinstein AR. Importance of events per independent variable in proportional hazards analysis I. Background, goals, and general strategy. J Clin Epidemiol. 1995;48:1495–501. https://doi.org/10.1016/0895-4356(95)00510-2.
Peduzzi P, Concato J, Feinstein AR, Holford TR. Importance of events per independent variable in proportional hazards regression analysis II. J Clin Epidemiol. 1995;48:1503–10.
Zou G. A modified Poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159:702–6. https://doi.org/10.1093/aje/kwh090.
Cats A, Jansen EPM, van Grieken NCT, Sikorska K, Lind P, Nordsmark M, et al. Chemotherapy versus chemoradiotherapy after surgery and preoperative chemotherapy for resectable gastric cancer (CRITICS): an international, open-label, randomised phase 3 trial. Lancet Oncol. 2018;19(5):616–628. https://doi.org/10.1016/S1470-2045(18)30132-3.
Piessen G, Messager M, Le Malicot K, Robb WB, Di Fiore F, Guilbert M, et al. Phase II/III multicentre randomised controlled trial evaluating a strategy of primary surgery and adjuvant chemotherapy versus peri-operative chemotherapy for resectable gastric signet ring cell adenocarcinomas—PRODIGE 19—FFCD1103—ADCI002. BMC Cancer. 2013. https://doi.org/10.1186/1471-2407-13-281.
Heger U, Sisic L, Nienhüser H, Blank S, Hinz U, Haag GM, et al. Neoadjuvant therapy improves outcomes in locally advanced signet-ring-cell containing esophagogastric adenocarcinomas. Ann Surg Oncol. 2018;25:2418–27. https://doi.org/10.1245/s10434-018-6541-3.
Li Y, Ma FH, Xue LY, Tian YT. Neoadjuvant chemotherapy vs upfront surgery for gastric signet ring cell carcinoma: a retrospective, propensity score-matched study. World J Gastroenterol. 2020;26:818–27. https://doi.org/10.3748/wjg.v26.i8.818.
Reynolds JV, Preston SR, O’Neill B, Baeksgaard L, Griffin SM, Mariette C, et al. ICORG 10–14: NEOadjuvant trial in Adenocarcinoma of the oEsophagus and oesophagoGastric junction International Study (Neo-AEGIS). BMC Cancer. 2017;17:1–10. https://doi.org/10.1186/s12885-017-3386-2.
Hoeppner J, Lordick F, Brunner T, Glatz T, Bronsert P, Röthling N, et al. ESOPEC: Prospective randomized controlled multicenter phase III trial comparing perioperative chemotherapy (FLOT protocol) to neoadjuvant chemoradiation (CROSS protocol) in patients with adenocarcinoma of the esophagus (NCT02509286). BMC Cancer. 2016;16:1–10. https://doi.org/10.1186/s12885-016-2564-y.
van Putten M, Nelen SD, Lemmens VEPP, Stoot JHMB, Hartgrink HH, Gisbertz SS, et al. Overall survival before and after centralization of gastric cancer surgery in the Netherlands. Br J Surg. 2018;105:1807–15. https://doi.org/10.1002/bjs.10931.
Jensen LS, Nielsen H, Mortensen PB, Pilegaard HK, Johnsen SP. Enforcing centralization for gastric cancer in Denmark. Eur J Surg Oncol. 2010;36:S50–4. https://doi.org/10.1016/j.ejso.2010.06.025.
Nelen SD, Heuthorst L, Verhoeven RHA, Polat F, Kruyt PM, Reijnders K, et al. Impact of centralizing gastric cancer surgery on treatment, morbidity, and mortality. J Gastrointest Surg. 2017;21:2000–8. https://doi.org/10.1007/s11605-017-3531-x.
Lee JH, Chang KK, Yoon C, Tang LH, Strong VE, Yoon SS. Lauren histologic type is the most important factor associated with pattern of recurrence following resection of gastric adenocarcinoma. Ann Surg. 2018;267:105–13. https://doi.org/10.1097/SLA.0000000000002040.
Smyth EC, Verheij M, Allum W, Cunningham D, Cervantes A, Arnold D, et al. Gastric cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27:v38–49. https://doi.org/10.1093/annonc/mdw350.
Acknowledgment
The authors would like to thank all participating hospitals in The Netherlands for collecting the data, and the NCR and PALGA for supplying the data for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Human Rights Statement and Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. This study was performed with nationwide, anonymous data; thus, informed consent or its substitute was waived by the Ethical Review Board of the NCR.
Disclosures
Relevant financial activities outside the submitted work. Peter D. Siersema is receiving research support from Pentax (Japan), The eNose Company, MicroTech (China) and Motus GI (USA). Rob H.A. Verhoeven has received research grants from Bristol-Myer Squibb and Roche. Emma C. Gertsen, Arjen van der Veen, Hylke J.F. Brenkman, Lodewijk A.A. Brosens, Rachel S. van der Post, Josianne C.H.B.M. Luijten, Pauline A.J. Vissers, Erik Vegt, Richard van Hillegersberg, and Jelle P. Ruurda have no disclosures to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gertsen, E.C., van der Veen, A., Brenkman, H.J.F. et al. Multimodal Therapy Versus Primary Surgery for Gastric and Gastroesophageal Junction Diffuse Type Carcinoma, with a Focus on Signet Ring Cell Carcinoma: A Nationwide Study. Ann Surg Oncol 31, 1760–1772 (2024). https://doi.org/10.1245/s10434-023-14690-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-023-14690-y